Health equity in telehealth access for Maryland residents

Offering telehealth services is not the same as offering equitable access. For many Maryland residents, a video visit is technically available but practically out of reach because of limited broadband, an outdated device, language barriers, or a coverage policy that doesn’t reimburse their specific situation. Telehealth access depends on a chain of components that must all work together, meaning that one broken link is enough to leave a patient without care. At Anchor Health, we see this reality every day, and we believe understanding the full picture is the first step toward changing it for families, women navigating health transitions, and adults managing chronic conditions across Maryland.
Table of Contents
- What does health equity in telehealth access mean?
- The multidimensional model of telehealth access
- Spotting disparities: who faces barriers in Maryland telehealth?
- Common edge cases: modality mismatch and the digital divide
- What most Marylanders miss about telehealth equity
- Connect with equitable telehealth care in Maryland
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Health equity goes beyond access | True equity means telehealth is usable for all Marylanders, not just available. |
| Digital divide impacts care | Connectivity, devices, and digital literacy create or close gaps in telehealth access. |
| Policy shapes outcomes | Maryland’s laws ensure telehealth coverage and audio-only options to support equitable care. |
| Modality matters for families | Matching telehealth tools to patients’ needs prevents mismatch and exclusion. |
What does health equity in telehealth access mean?
With the basic context set, let’s clarify what health equity actually entails when it comes to telehealth. Health equity is not simply the absence of discrimination. It means every person can obtain appropriate care regardless of race, income, language, age, or ZIP code, and that non-clinical barriers are actively removed rather than quietly tolerated.
A common misconception is that making telehealth available automatically makes it equitable. Availability is one condition, not the whole answer. A rural family in Garrett County, Maryland may have a telehealth platform login but no reliable internet connection. A Spanish-speaking parent in Prince George’s County may have high-speed broadband but receive care from a provider who offers no language support. In both cases, telehealth exists on paper but fails in practice.
Telehealth access depends on a chain of components that includes the technology infrastructure, the patient’s ability to use it, the provider’s capacity to meet the patient’s needs, and the payment system that sustains it. Each component must be present and functioning for access to be genuinely equitable.
In Maryland, key barriers include:
- Broadband gaps in rural counties like Allegany, Caroline, and Somerset
- Device access limitations among older adults and low-income households
- Low digital literacy affecting seniors and adults with limited formal education
- Language barriers for Spanish, French Creole, and Amharic-speaking communities
- Insurance coverage gaps that exclude certain telehealth modalities
- Distrust of technology-based care rooted in historical mistreatment by healthcare systems
“Health equity in telehealth is not a technology problem alone. It is a social, economic, and policy problem that technology can either worsen or help solve, depending on how it is implemented.”
Recognizing these layered barriers is what separates genuine equity work from simply checking a box.
The multidimensional model of telehealth access
Having defined health equity, we can zoom into the framework for measuring and improving telehealth access. Researchers and policymakers use a structured approach built around multiple dimensions of healthcare access, and understanding this model helps you ask better questions about whether your care is truly accessible.
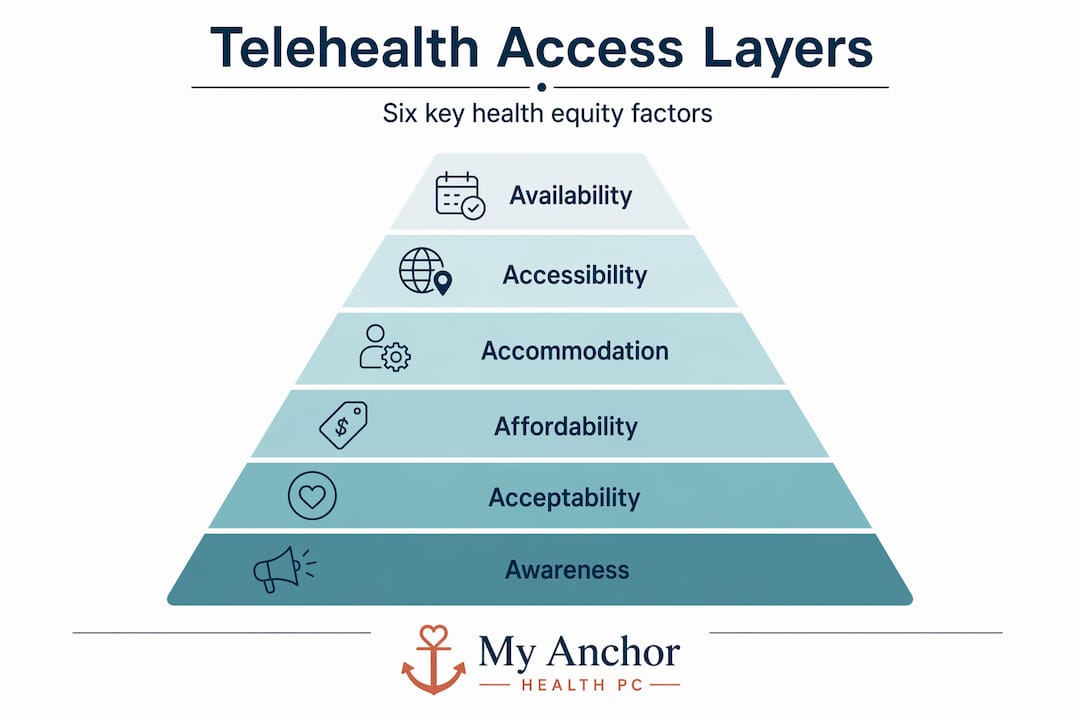
A review of reviews frames healthcare access as multidimensional, typically organized around six dimensions. These are often called the six “A” dimensions: Availability, Accessibility, Affordability, Acceptability, Adequacy, and Awareness. Digital determinants of health, such as broadband quality, device ownership, digital literacy, language compatibility, and technology cost, map directly onto each of these dimensions.
| Access dimension | What it means | Digital determinant that affects it |
|---|---|---|
| Availability | Services exist and are offered | Provider offers telehealth platform |
| Accessibility | Patient can physically or technically reach the service | Broadband speed and device quality |
| Affordability | Patient can pay for the service | Data plan costs, copays, coverage rules |
| Acceptability | Patient trusts and is comfortable with the service | Cultural fit, language, provider familiarity |
| Adequacy | The service meets clinical need appropriately | Modality match, clinical scope of telehealth |
| Awareness | Patient knows the service exists and how to use it | Health literacy, outreach, digital navigation support |
For Maryland families, the dimensions most commonly disrupted are accessibility (broadband and device), affordability (data costs and insurance gaps), and awareness (not knowing what telehealth covers or how to navigate it). Providers and policymakers who want to improve equity should start here.
Key digital determinants affecting Maryland telehealth users:
- Broadband access: Rural and some urban zip codes lack consistent high-speed internet
- Device ownership: Shared household devices create privacy and scheduling challenges
- Digital literacy: Patients unfamiliar with video platforms need guided onboarding
- Language support: Platforms and providers without multilingual capacity lose patients at the awareness and acceptability levels
- Data costs: Patients on limited mobile data plans may avoid video visits to protect their data budget
Pro Tip: Before your first telehealth visit, ask your provider whether audio-only appointments are available as a backup. Audio-only care is often reimbursable in Maryland and can bridge the gap when your internet connection is unstable or your device camera doesn’t work.
Spotting disparities: who faces barriers in Maryland telehealth?
With the framework in mind, next let’s identify who in Maryland is most affected by telehealth access inequities. The data is clear, and it points to patterns that demand honest attention.
Empirical evidence shows disparities in telehealth use across racial, geographic, and insurance lines. Black, Hispanic, and low-income patients are less likely to successfully complete a telehealth visit compared to white, higher-income patients, even when controlling for clinical need. Telehealth does not automatically level the playing field. Without intentional policy and practice design, it can widen existing gaps.

Here is a look at how access gaps compare across care settings for key Maryland populations:
| Population group | In-person access challenges | Telehealth access challenges | Where equity gaps persist |
|---|---|---|---|
| Rural Maryland residents | Distance, transportation | Broadband gaps | Accessibility dimension |
| Medicaid enrollees | Limited accepting providers | Coverage rules on modality | Affordability dimension |
| Women in perimenopause | Rushed or dismissed care | Fragmented follow-up | Adequacy dimension |
| Older adults (65+) | Mobility limitations | Digital literacy barriers | Awareness and accessibility |
| Non-English speakers | Language access gaps | Platform and provider language limits | Acceptability dimension |
Women navigating health transitions like perimenopause face a particular combination of challenges. Their care needs are often ongoing, require nuanced follow-up, and can be dismissed or minimized in both in-person and telehealth settings. Without a consistent provider who knows their history, important patterns go unnoticed.
Adults managing chronic conditions such as hypertension, diabetes, or obesity benefit from continuity of care. For Medicaid enrollees, however, coverage rules have historically restricted which telehealth modalities qualify for reimbursement. This means a patient whose only option is an audio call may not have that visit covered at all.
Maryland has made meaningful progress on this front. Key policy achievements include:
- Telehealth parity law: Maryland requires that telehealth services are covered regardless of the patient’s physical location at the time of the visit, removing the longstanding “originating site” restriction.
- Audio-only reimbursement: Maryland policy supports reimbursement for audio-only visits in clinical contexts where audio-visual technology is unavailable or inappropriate.
- Medicaid telehealth expansion: Maryland Medicaid has expanded coverage of telehealth services to include a broader range of providers and service types.
- Interstate compact participation: Maryland’s participation in provider licensing compacts supports access for patients who move or split time between states.
These policy wins matter because they shift the structural environment. But policy on paper still needs providers who actively build their care model around these protections and communicate them clearly to patients.
Common edge cases: modality mismatch and the digital divide
Understanding who faces barriers allows us to dive into specific scenarios that matter for Maryland telehealth users. Two situations come up again and again: modality mismatch and digital divide failures.
Telehealth digital divide edge cases include scenarios where the technology format offered does not match the patient’s actual capabilities or clinical needs. This is modality mismatch, and it is more common than most people realize.
Consider these real scenarios Maryland patients face:
- A patient schedules a video visit but their only internet access is a slow mobile hotspot. The video call drops repeatedly. The provider documents the visit as incomplete.
- An elderly woman needs to discuss a sensitive mental health concern. The video platform requires a smartphone app she cannot install because her phone is too old. She cancels rather than troubleshoot.
- A parent tries to connect their child for a pediatric visit on a household laptop that is also being used by other family members for work and school. They cannot find a private, quiet space during business hours.
- A Medicaid patient calls for an audio-only visit. The provider’s billing system is not set up to submit audio-only claims, and the patient is told they need to reschedule as a video visit.
Each of these is a health equity failure. The care was technically available but practically inaccessible.
Practical fixes Maryland families and patients can take:
- Ask explicitly about audio-only options when scheduling, especially if your broadband is unreliable
- Request a technology check-in before your appointment if you are new to video visits
- Ask about language interpretation services if English is not your primary language
- Confirm what your insurance covers before your first visit, including whether audio-only is reimbursed
- Find out if the provider offers flexible scheduling to accommodate shared device households or working adults
- Look for providers who actively explain your rights under Maryland’s telehealth coverage laws
Pro Tip: If your video connection fails during a visit, do not simply give up. Call your provider’s office directly and ask whether the appointment can continue by phone. Many Maryland providers can switch to audio-only mid-visit without requiring a separate appointment or additional copay.
The digital divide is not just about access to technology. It is about confidence, language, privacy, and cost. Providers who understand this design their care model accordingly.
What most Marylanders miss about telehealth equity
Here is something we see repeatedly in conversations with patients: many people assume that once they have figured out how to log into a video visit, the equity problem is solved. It is not. Getting connected is one step. Getting appropriate, consistent, high-quality care through that connection is a different challenge entirely.
Equity in telehealth requires matching modality, coverage, and patient support to actual barriers so that access is determined by clinical need rather than social circumstance. A provider who only offers video, only accepts certain insurance types, and never asks whether a patient understood their care plan has not achieved equity, even if the technology works perfectly.
We also notice that equity conversations in telehealth tend to focus heavily on rural communities and broadband gaps. Those are real and important problems. But urban and suburban Maryland residents face their own equity gaps, including provider distrust rooted in documented histories of medical mistreatment, language barriers in high-density immigrant communities, and coverage restrictions that affect people on Medicaid even in well-connected ZIP codes.
True equity requires providers to ask the questions that most systems skip. Does this patient trust us enough to be honest about their symptoms? Do they know what their insurance actually covers for telehealth? Do they have a private space for this conversation? Have we made it easy for them to reach us if something is unclear after the visit?
These are not technology questions. They are relationship questions. And that is exactly why relationship-based primary care, built on continuity and trust, is not a premium option but a core equity strategy.
Connect with equitable telehealth care in Maryland
If this article raises questions about whether your own healthcare is meeting your real needs, you are asking exactly the right thing. Anchor Health was built to address the gaps that standard telehealth models leave behind, including rushed visits, fragmented care, and providers who don’t know your history.
We work with Maryland families, women navigating health transitions, and adults managing ongoing conditions through our Anchored Care℠ᴵᴾ model, which prioritizes relationship, continuity, and time. Whether you are looking for thoughtful support around perimenopause guidance, management of a chronic condition, or just a primary care provider who will actually listen, we are here for that. We accept insurance, offer membership options, and provide secure video visits across Maryland. Reaching equitable, personalized care should not require navigating a system alone. We make it straightforward.
Frequently asked questions
What barriers most affect telehealth access in Maryland?
Maryland residents face barriers like limited broadband, device access, low digital literacy, and reimbursement gaps, since telehealth access depends on a chain of components that must all work together for care to be genuinely accessible.
How do Maryland policies support health equity in telehealth?
Maryland telehealth law and policy ensures services are covered regardless of where the patient is located and includes support for audio-only visits when video technology is unavailable, removing two major structural barriers to equitable access.
Is audio-only telehealth available and reimbursed in Maryland?
Yes, Maryland policy supports audio-only reimbursement in relevant clinical contexts, which is especially important for patients without reliable video-capable devices or internet connections.
Can telehealth widen equity gaps?
Without targeted policies and intentional provider practices, telehealth may widen gaps for groups that lack digital tools, affordable data plans, or coverage that recognizes non-video visit modalities.
Recommended
Blog & Information Disclaimer
Last Updated: May 23, 2026
The information provided on the Anchor Health website (https://myanchorhealthpc.com/), including but not limited to blog posts, articles, newsletters, graphics, and other materials (collectively, the "Content"), is for general informational and educational purposes only.
By accessing and using this website, you acknowledge and agree to the following terms and conditions:
The Content on this website is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician, nurse practitioner, or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Reading, interacting with, or sharing the Content on this website does not establish a patient-provider relationship between you and Anchor Health or any of its clinicians, including Paule Valery Joseph, PhD, MBA, CRNP, FAAN. A formal patient-provider relationship is only established after you have completed the formal intake process, signed our clinical consent forms, and participated in a secure clinical consultation.
If you are experiencing a medical emergency, call 911 or seek emergency medical services immediately.
Anchor Health is a primary care practice and does not provide emergency or crisis intervention services through its website or blog.
While Anchor Health strives to provide thoughtful, evidence-based information grounded in our Anchored Care℠ model, healthcare is a rapidly evolving field. We make no representations or warranties, express or implied, about the completeness, accuracy, reliability, or suitability of the information contained in the Content. Any reliance you place on such information is strictly at your own risk.
Anchor Health is a telehealth practice providing services to patients physically located within the state of Maryland. The information provided on this blog is intended for residents of Maryland and is governed by the laws and regulations of that state. Accessing this information from outside of Maryland does not imply that our clinicians are licensed to practice medicine or provide consultations in your jurisdiction.
Content related to Weight & Metabolic Health, including discussions of GLP-1 medications or other medical therapies, is provided for educational context regarding our clinical approach. Prescriptions and specific medical recommendations are only made following a comprehensive clinical evaluation, diagnostic testing, and shared decision-making within a formal patient-provider relationship.
This website may contain links to external websites that are not provided or maintained by or in any way affiliated with Anchor Health. Please note that Anchor Health does not guarantee the accuracy, relevance, timeliness, or completeness of any information on these external websites.
To the fullest extent permitted by law, Anchor Health, its owners, and its employees shall not be liable for any direct, indirect, incidental, consequential, or punitive damag
Related posts


